Some Smaller Hospitals Can Deliver Big Savings | Report: No link between costs and quality of care
As the state moves slowly forward on efforts to control health care costs, a recent study by the Massachusetts Division of Health Care Finance and Policy provides another boost to the argument that smaller community hospitals tend to provide many types of care as well as, and significantly more cheaply than, their larger counterparts.
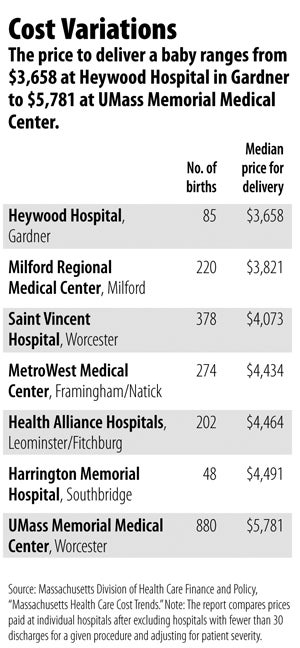
In Central Massachusetts, two hospitals that stacked up particularly well in the study were Heywood Hospital in Gardner and Milford Regional Medical Center.
The two hospitals say they’ve made a concerted effort to keep their prices down. But low reimbursement rates are a paradox, representing both an increasingly valuable selling point and an obvious blow to the revenue stream.
Size Matters
The report, Price Variation in Health Care Services, examined the dollar amount billed to private insurers for treating specific conditions and found that a given procedure was often nearly twice as expensive at one hospital as another, even when controlled for the severity of the medical case.
It found no correlation between price and quality of care.
The data the study provides is limited because in many cases small hospitals don’t perform a given procedure enough times at a given severity level to draw valid comparisons.
Traditional, non-C-section delivery of a baby was the only procedure common enough to offer a comparison between the largest and smallest Central Massachusetts hospitals, and the difference is striking. At Heywood, the median price for a delivery is $3,658. At Milford, it’s $3,821. At UMass Memorial Medical Center, the most expensive hospital in the area, it’s $5,781.
The division’s acting commissioner, Seena Perumal Carrington, said it’s not possible to extrapolate from the delivery numbers to other procedures, but she noted that in general small community hospitals provide care less expensively than larger facilities.
Lorie Martiska, vice president of community relations and development at Heywood, said the hospital’s position in the state study isn’t surprising.
“Over many years we have tried to be as lean as we possibly can, and I think we are extremely lean, but still delivering great quality of care,” she said.
Martiska said Heywood has pushed for greater efficiencies in administration and other non-patient-care departments in an effort to keep costs down without sacrificing quality.
At Milford, President Edward J. Kelly said keeping quality high is actually a route to keeping costs down.
“How Milford has been able to stay independent and really thrive over the last couple decades is we’ve been building, expanding,” he said.
Thanks to that expansion, as well as high-tech equipment, top-level staff and some partnerships with larger hospitals, Kelly said, the hospital has been able to attract more patients, sometimes hitting capacity. The relatively high patient volume helps make the numbers work.
Rate Comparisons
So if quality of care doesn’t explain why some hospitals are more expensive than others, what does? The state study rejects the explanation that higher private-insurance reimbursement rates make up for the relatively low rates paid by Medicare and Medicaid, noting that hospitals with high numbers of patients on the government plans aren’t particularly likely to charge private insurers more.
It also considers the idea that high area wages, indirect medical education, treating low-income patients, high-cost technologies or costly outlier cases drive higher rates. The report gives reason to doubt that rationale — it notes that Medicare rates explicitly consider those factors, yet hospitals with higher reimbursement to Medicare aren’t necessarily the same ones that have higher private-payer rates. Carrington says the question is a complicated one since it’s hard to know what factors hospitals and private insurers take into account when they negotiate reimbursement rates.
A 2010 study by Attorney General Martha Coakley’s office came to the conclusion that some hospitals get paid more primarily because they have market leverage. In other words, large hospitals negotiate higher reimbursement rates from private insurers because they can.
The corollary to that, of course, is that lower-cost hospitals are lower-cost because they don’t have the clout to negotiate higher rates.
Martiska said that’s certainly something that concerns Heywood.
“Frankly, hospitals are starting to get squeezed from all sides,” she said.
Kelly at Milford Regional said changes by insurers are playing out to the lower-cost hospitals’ advantage as more patients take high-deductable plans that cause them to feel the pain of higher costs.
He said many hospitals are also watching the state debate over health care costs in the hope that the process of negotiating reimbursement rates will be totally revamped. Instead of starting with current rates and making incremental changes from there, he said, insurers and hospitals should start fresh.
“The new baseline needs to be everyone being paid the same,” he said.
WBJ Web Partners
Most Recent



Most Recent






0 Comments